2026: Volume 5, Issue 1
Current Issue
 Abstract
Abstract  PDF
PDFKnowledge and Practice of Healthcare Providers on Intravenous Fluid Stewardship in Pediatric Intensive Care Units: A Cross-Sectional Study from Alexandria
Dina Hamdy Selim1*, Alaa Elsaied Mohamed2 , Nada Roshdy Abdellah2
1Fellow of Clinical Nutrition, Alexandria University Hospital, Alexandria University, Egypt
2Clinical Pharmacist in Talaba Sportiong Hospital and Shatby Pediatric Hospital, Alexandria , Egypt
*Corresponding author: Dina Hamdy Selim, PhD, Fellow of Clinical nutrition, Al Mawasah University Hospital, Educational and Medical Complex, Alexandria University, Alexandria 21526; Egypt, Phone: +201224020689, E-mail: [email protected]
Received : October 20, 2025 Published : March 15, 2026
Citation: Selim DH, et al. (2026). Knowledge and Practice of Healthcare Providers on Intravenous Fluid Stewardship in Pediatric Intensive Care Units: A Cross-Sectional Study from Alexandria. Nutraceutical Res. 5(1):20.
Copyright: Selim DH, et al. © (2026).
ABSTRACT
Introduction: Intravenous fluid (IV) therapy is integral to the management of critically ill children in pediatric intensive care units (PICUs), given their frequent inability to maintain adequate oral intake. However, inappropriate prescribing and administration of IV fluids are associated with significant morbidity and mortality, particularly in pediatric patients who are more susceptible to complications such as fluid overload, infiltration, and electrolyte imbalances. Aim of the study: To assess the knowledge and practice of healthcare providers regarding IV fluid administration and stewardship in the PICU settings of Alexandria Pediatric Hospitals (Shatby and Talaba hospitals), and to identify associated barriers, training gaps, and areas requiring stewardship interventions. Methods: A cross-sectional observational study was conducted among 128 healthcare providers comprising 56 nurses, 21 physicians, and 51 pharmacists working in the PICUs of two Alexandria hospitals. Data were collected using a validated questionnaire assessing basic knowledge, prescribing and administration practices, awareness of complications, training history, and perceived barriers to implementing fluid stewardship. Knowledge adequacy was defined as correctly answering ≥ 60% of knowledge-domain items. Descriptive and comparative analyses were performed using SPSS v20, applying Chi-square and Monte Carlo correction tests where appropriate (p < 0.05). Results: Only 35% of nurses, 23% of physicians, and 52% of pharmacists correctly answered basic knowledge questions regarding IV fluids. While physicians demonstrated comparatively better clinical monitoring practices, substantial knowledge–practice gaps were observed across all professional groups. Notably, 80.4% of nurses and 64.7% of pharmacists identified fluid overload as the most frequent complication. Only 55.4% of nurses and 25.5% of pharmacists had received specific training in IV fluid stewardship. Limitations include the single-region design and reliance on self-reported data. Conclusion: Structured fluid stewardship programs integrating physicians, nurses, and pharmacists are essential to improve safety in pediatric IV fluid therapy. Targeted educational initiatives and policy-driven implementation strategies should be prioritized to reduce preventable complications.
Keywords: Intravenous Fluids, Pediatric Intensive Care Unit, Fluid Stewardship, Healthcare Providers, Knowledge Assessment, Egypt
INTRODUCTION
Intravenous (IV) fluids are among the most frequently prescribed medications in both adult and pediatric clinical settings, particularly in intensive care units where oral intake is impossible due to impaired consciousness or gastrointestinal dysfunction. Mismanagement of IV fluid prescribing is well-documented to increase patient morbidity and mortality, underscoring the importance of rational and evidence-based fluid therapy [1].
Complications of IV fluid administration include infiltration, hematoma, air embolism, phlebitis, extravascular drug administration, and intraarterial injection. Although intraarterial injection is rare, it carries life-threatening consequences [2]. Adverse effects of crystalloids span a wide clinical spectrum: from relatively mild manifestations such as headache and hypertension, to severe outcomes including pulmonary edema, heart dysfunction, anaphylactic reactions, acute kidney injury, coagulopathy due to haemodilution, hypothermia, thrombophlebitis, and metabolic acidosis. Hypotonic solutions and normal saline carry specific risks; the latter is associated with metabolic acidosis and renal impairment, while both can aggravate brain swelling, elevated intracranial pressure, and neurological morbidity [3,4].
In the pediatric population, IV therapy is further complicated by anatomical and physiological factors: small-caliber and difficult-to-access veins, limited patient cooperation, parental anxiety, and increased subcutaneous adiposity. These factors increase the complexity of venipuncture and challenge the fixation and maintenance of IV access [5-9].
Patient monitoring during IV fluid therapy is critical and encompasses fluid balance assessment, outcome-guided evaluation, and goal-directed fluid therapy. Hemodynamic parameters such as arterial pressure, central venous pressure, and urinary output are commonly utilized, though they are recognized as imprecise indicators of appropriate fluid loading [4].
Each professional group within the healthcare team plays a distinct and essential role in IV fluid management. Nurses are primarily responsible for therapy implementation, venipuncture, technical administration procedures, and front-line monitoring for complications [3]. Pharmacists contribute through reviewing patient files, calculating fluid requirements, dispensing, ensuring compatibility and stability of IV formulations, and conducting pharmacovigilance activities [4-7]. Physicians bear primary prescribing responsibility and are expected to apply clinical guidelines and adjust therapy in response to patient outcomes.
Fluid stewardship is defined as a series of coordinated, multidisciplinary interventions aimed at ensuring judicious IV fluid administration. It requires a thorough understanding of pharmacokinetics and pharmacodynamics, as well as clarity on indications, contraindications, dosing, duration, and de-escalation strategies — encapsulated in the 4 D's: drug, dosing, duration, and de-escalation [1]. Prescription review is guided by the 5 P's: prescriber, prescription, pharmacy, preparation, and patient.
A well-functioning fluid stewardship team should include physicians, nurses, clinical pharmacists, and dietitians. The primary goal of such a program is to maximize clinical outcomes and minimize fluid-related complications; the secondary goal is to reduce healthcare costs through more rational utilization of IV fluids [1]. Global literature, including work by Malbrain et al. [1], highlights that stewardship goals are best achieved through improvements in prescribing practice, development of robust and regularly updated guidelines, rolling multidisciplinary education programs, and systematic quality assurance measures.
Morbidity and mortality among hospitalized patients can be significantly increased by errors arising from inadequate knowledge and suboptimal practice in IV fluid therapy. The present study therefore assessed the knowledge, practices, and perceived barriers of nurses, pharmacists, and physicians working in pediatric ICUs in Alexandria, Egypt.
METHODOLOGY
Study Design
A cross-sectional observational study was conducted in the PICUs of two Alexandria pediatric hospitals: Shatby Pediatric University Hospital and Talaba Sporting Hospital.
Sample Size and Participants
Sample size was calculated using G*Power software, assuming an effect size of 0.25, alpha error of 0.05, and a study power of 80%, yielding a minimum required sample of 128 participants. A total of 128 healthcare providers (21 physicians, 56 nurses, and 51 pharmacists) working in the ICU and CCU of both hospitals were enrolled. Convenience sampling was used; all available healthcare staff meeting inclusion criteria were invited to participate.
Data Collection Tool
Data were collected using a validated questionnaire [10-12] assessing basic knowledge of IV fluids, prescribing and administration practices, awareness of complications, training history, and perceived barriers to stewardship implementation. Thirty-six questionnaires were administered via online Google Form [13] and 92 were completed in written format. Data collection commenced following receipt of institutional permissions and written informed consent to access both hospitals. Adequate knowledge was defined as correctly answering ≥60% of knowledge-domain items. The study adheres to STROBE guidelines for cross-sectional studies.
Ethics
The study protocol was approved by the Ethics Committee, Faculty of Medicine, Alexandria University (IRB No.: 0001298; FWA No.: 00018699). An oral informed consent was taken from all participants , Participant confidentiality was maintained throughout data collection and analysis. Self-reporting bias is acknowledged as an inherent limitation of the study design.
Statistical Analysis
Data were entered and analyzed using IBM SPSS software package version 20.0 (Armonk, NY: IBM Corp, 2011). Qualitative variables were described using frequency and percentage. Between-group comparisons were performed using the Chi-square test for categorical variables, and the Monte Carlo correction was applied when more than 20% of expected cell counts fell below 5. Statistical significance was set at p < 0.05.
RESULTS
A total of 128 healthcare providers participated: 56 nurses (43.8%), 21 physicians (16.4%), and 51 pharmacists (39.8%), as illustrated in Figure 1.
.png)
Figure 1: Distribution of the Three Studied Groups
Table 1A: Comparison between the three studied groups to assess the practice in the usage of IV fluids in the units
| Q | Nurses (n = 56) | Physician (n = 21) | Pharmacist (n = 51) | χ² | p | |||
| No. | % | No. | % | No. | % | |||
| Q15: Do you consider IV fluid prescription potentially dangerous if not done properly? | MCp<0.001* | |||||||
| Always | ||||||||
| 25 | 44.6 | 8 | 38.1 | 40 | 78.4 | * | ||
| 22.584 | ||||||||
| Sometimes | 23 | 41.1 | 13 | 61.9 | 11 | 21.6 | ||
| Never | 8 | 14.3 | 0 | 0 | 0 | 0 | ||
| Q16: Do you assess for risk of fluid overload before IV fluids prescription? | MCp=0.002* | |||||||
| Always | ||||||||
| 38 | 67.9 | 21 | 100 | 32 | 62.7 | * | ||
| 15.174 | ||||||||
| Sometimes | 18 | 32.1 | 0 | 0 | 16 | 31.4 | ||
| Never | 0 | 0 | 0 | 0 | 3 | 5.9 | ||
Table 1B: Comparison between the three studied groups to assess the practice in the usage of IV fluids in the units
| Q | Nurses (n = 56) | Physician (n = 21) | Pharmacist (n = 51) | χ² | p | |||
| No. | % | No. | % | No. | % | |||
| Q26: How confident are you managing IV fluid therapy in pediatrics? | <0.001* | |||||||
| * | ||||||||
| Very Confident | ||||||||
| 31 | 55.4 | 12 | 57.1 | 4 | 7.8 | 33.196 | ||
| Somewhat Confident | 17 | 30.4 | 9 | 42.9 | 37 | 72.5 | ||
| Not Confident | 8 | 14.3 | 0 | 0 | 10 | 19.6 | ||
| Q28: Are you familiar with local or international guidelines for IV fluid therapy in children (e.g., NICE, AAP)? | 0.004* | |||||||
| Yes | * | |||||||
| 37 | 66.1 | 20 | 95.2 | 28 | 54.9 | 10.854 | ||
| No | 19 | 33.9 | 1 | 4.8 | 23 | 45.1 | ||
| Q29: Which type of IV fluids do you most commonly prescribe for pediatric patients? | MCp<0.001* | |||||||
| Isotonic | ||||||||
| * | ||||||||
| 44 | 78.6 | 12 | 57.1 | 42 | 82.4 | 23.646 | ||
| Hypotonic | 3 | 5.4 | 9 | 42.9 | 4 | 7.8 | ||
| Balanced Crystalloid | 9 | 16.1 | 0 | 0 | 5 | 9.8 | ||
| Q30: How often do you monitor electrolytes (e.g., sodium, potassium) when administering IV fluids? | 0.107 | |||||||
| Always | ||||||||
| 17 | 30.4 | 5 | 23.8 | 15 | 29.4 | 7.62 | ||
| Sometimes | 22 | 39.3 | 3 | 14.3 | 19 | 37.3 | ||
| Never | 17 | 30.4 | 13 | 61.9 | 17 | 33.3 | ||
| Q31: Signs of fluid overload (e.g., edema, respiratory distress) | MCp=0.001* | |||||||
| Always | * | |||||||
| 5 | 8.9 | 5 | 23.8 | 18 | 35.3 | 19.443 | ||
| Sometimes | 46 | 82.1 | 12 | 57.1 | 21 | 41.2 | ||
| Never | 5 | 8.9 | 4 | 19 | 12 | 23.5 | ||
| Q32: What resources do you primarily use for IV fluid therapy decisions? | MCp<0.001* | |||||||
| Clinical guidelines (NICE, AAP) | * | |||||||
| 16 | 28.6 | 12 | 57.1 | 27 | 52.9 | 50.245 | ||
| Hospital protocols | 39 | 69.6 | 1 | 4.8 | 12 | 23.5 | ||
| Colleagues/mentors | 1 | 1.8 | 1 | 4.8 | 8 | 15.7 | ||
| Medical literature | 0 | 0 | 7 | 33.3 | 4 | 7.8 | ||
χ²: Chi-square test MC: Monte Carlo p: p value for comparing between the three studied groups *: Statistically significant at p ≤ 0.05
Table 2: Comparison between the three studied groups about Complications on the usage of IV fluids
| Q | Nurses (n = 56) | Physician (n = 21) | Pharmacist (n = 51) | χ² | p | |||
| No. | % | No. | % | No. | % | |||
| Q18: Have you encountered any IV fluid-related complications (e.g., hyponatremia, fluid overload)? | 0.017* | |||||||
| Yes | ||||||||
| 46 | 82.1 | 17 | 81 | 30 | 58.8 | 8.176* | ||
| No | 10 | 17.9 | 4 | 19 | 21 | 41.2 | ||
| Q19: What is the most common complication? | MCp<0.001* | |||||||
| Anaphylaxis | * | |||||||
| 9 | 16.1 | 18 | 85.7 | 16 | 31.4 | 31.797 | ||
| Fluid overload | 45 | 80.4 | 3 | 14.3 | 33 | 64.7 | ||
| Hyponatremia | 2 | 3.6 | 0 | 0 | 2 | 3.9 | ||
| Q20: How often do patients suffer from fluid overload? | MCp<0.001* | |||||||
| * | ||||||||
| Always | ||||||||
| 4 | 7.1 | 14 | 66.7 | 40 | 78.4 | 66.682 | ||
| Sometimes | 48 | 85.7 | 7 | 33.3 | 9 | 17.6 | ||
| Never | 4 | 7.1 | 0 | 0 | 2 | 3.9 | ||
| Q21: How often do patients suffer from extravasation? | <0.001* | |||||||
| * | ||||||||
| Always | ||||||||
| 5 | 8.9 | 2 | 9.5 | 32 | 62.7 | 76.639 | ||
| Sometimes | 46 | 82.1 | 6 | 28.6 | 16 | 31.4 | ||
| Never | 5 | 8.9 | 13 | 61.9 | 3 | 5.9 | ||
| Q22: How often do patients suffer from hyponatremia? | MCp<0.001* | |||||||
| * | ||||||||
| Always | ||||||||
| 11 | 19.6 | 9 | 42.9 | 8 | 15.7 | 18.43 | ||
| Sometimes | 36 | 64.3 | 9 | 42.9 | 43 | 84.3 | ||
| Never | 9 | 16.1 | 3 | 14.3 | 0 | 0 | ||
| Q23: Which type of complication is more common? | <0.001* | |||||||
| * | ||||||||
| Fluid-related (saline, glucose) | ||||||||
| 32 | 57.1 | 21 | 100 | 26 | 51 | 16.011 | ||
| Technique-related (line-related) | 24 | 42.9 | 0 | 0 | 25 | 49 | ||
χ²: Chi-square test MC: Monte Carlo p: p value for comparing between the three studied groups *: Statistically significant at p ≤ 0.05
Table 3: Comparison between the three studied groups about Training and Implementation of Stewardship
| Q | Nurses (n = 56) | Physician (n = 21) | Pharmacist (n = 51) | χ² | p | |||
| No. | % | No. | % | No. | % | |||
| Q24: Have you received any specific training on IV fluid stewardship? | MCp=0.002* | |||||||
| * | ||||||||
| Yes | ||||||||
| 31 | 55.4 | 13 | 61.9 | 13 | 25.5 | 12.709 | ||
| No | 25 | 44.6 | 8 | 38.1 | 38 | 74.5 | ||
| Q25: Do you apply IV fluid stewardship? | MCp=0.007* | |||||||
| * | ||||||||
| Yes | ||||||||
| 30 | 53.6 | 18 | 85.7 | 39 | 76.5 | 10.062 | ||
| No | 26 | 46.4 | 3 | 14.3 | 12 | 23.5 | ||
χ²: Chi-square test MC: Monte Carlo p: p value for comparing between the three studied groups *: Statistically significant at p ≤ 0.05
Table 4: Comparison between the three studied groups according to Barriers facing the implementation of Stewardship
| Q | Nurses (n = 56) | Physician (n = 21) | Pharmacist (n = 51) | χ² | p | |||
| No. | % | No. | % | No. | % | |||
| Q33: What barriers do you face when implementing IV fluid stewardship? | ||||||||
| (Check all that apply)Lack of time | ||||||||
| 14 | 25 | 0 | 0 | 15 | 29.4 | 7.655* | ||
| 0.022* | ||||||||
| Lack of guidelines | 13 | 23.2 | 4 | 19 | 20 | 39.2 | ||
| Uncertainty about fluid choice | 7 | 12.5 | 0 | 0 | 8 | 15.7 | ||
| Difficulty monitoring patients | 8 | 14.3 | 5 | 23.8 | 4 | 7.8 | ||
| All of the above | 17 | 30.4 | 12 | 57.1 | 19 | 37.3 | ||
χ²: Chi-square test p: p value for comparing between the three studied groups *: Statistically significant at p ≤ 0.05
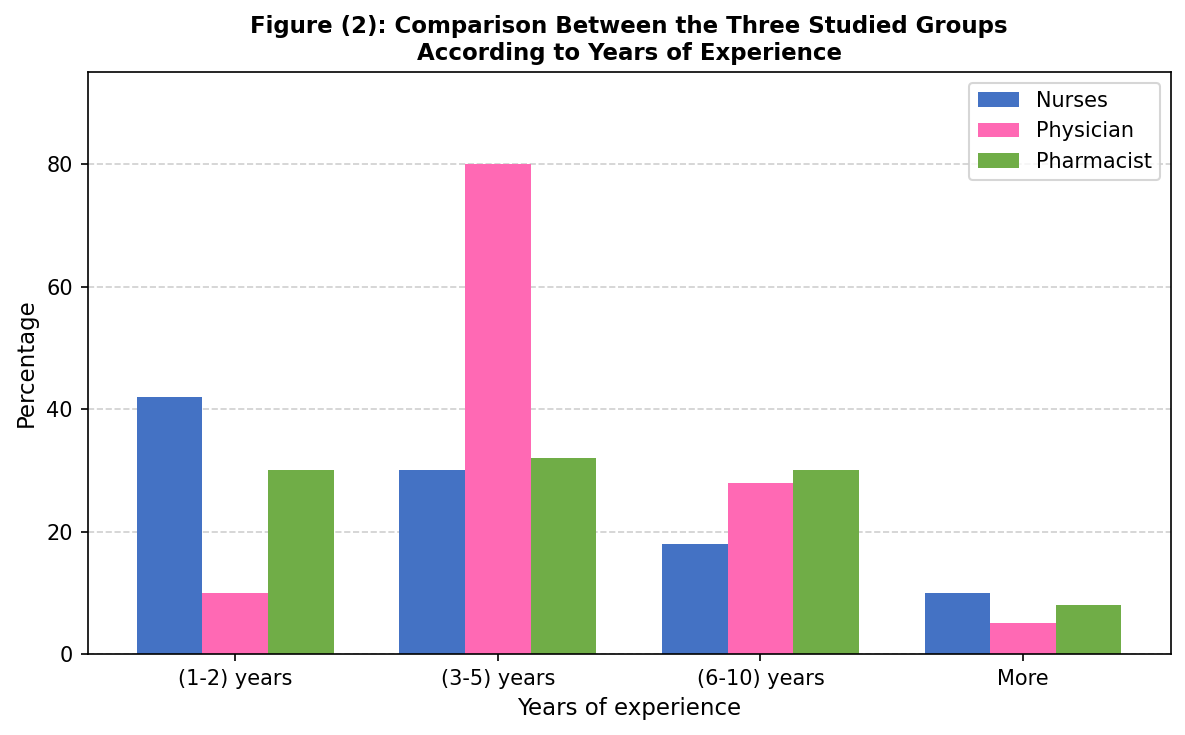
Figure 2: Comparison between the Three Studied Groups According to Years of Experience
Table 1 [Questions 15–17 and 26–32] assesses the IV fluid management practices of healthcare providers across the three groups. Among nurses, responses ranged between 'always' and 'sometimes,' indicating inconsistent adherence to recommended procedures — an inconsistency that underscores the need for a formal stewardship framework to standardize and regulate these processes.
Approximately 30% of nurses reported being only somewhat confident in managing IV fluid therapy, a proportion that is clinically significant and cannot be overlooked. The majority (66%) of nurses were familiar with local or international guidelines (NICE, AAP), highlighting the potential value of structured educational programs. Furthermore, 69% of nurses rely primarily on hospital protocols when making IV fluid decisions, while only 1.8% consult mentors or colleagues.
Physician responses in Table 1 showed higher rates of formal assessment, monitoring, and follow-up of IV fluid therapy compared to nurses, suggesting a comparatively greater degree of clinical vigilance. Nevertheless, only 38% of physicians consistently recognized the potential severity of IV fluid-related adverse events, indicating that stewardship awareness should be reinforced across all prescribing groups.
Table 2 assesses IV fluid complications. Fluid overload was identified as the most common complication by 80.4% of nurses, 85.7% of physicians, and 64.7% of pharmacists. Extravasation and hyponatremia were also reported as significant complications, particularly relevant in the pediatric population. Among pharmacists, 78.4% acknowledged the serious consequences of inadequately managed IV fluid therapy, reflecting their potential contribution to pharmacovigilance within the stewardship team.
Table 3 demonstrates important training gaps. Approximately 44.6% of nurses had not received any specific IV fluid stewardship training, and 74.5% of pharmacists lacked such training, with 23.5% reporting they do not apply any stewardship principles in practice. A higher proportion of physicians (61.9%) had received specific training and reported applying formal protocols based on clinical guidelines.
Table 4 identifies barriers to stewardship implementation. The most frequently cited single barrier among nurses and pharmacists was lack of time (25% and 29.4%, respectively). A substantial proportion of all groups endorsed all listed barriers collectively — physicians: 57.1%; pharmacists: 37.3%; nurses: 30.4% — suggesting that systemic, multidisciplinary approaches are needed to overcome these obstacles.
DISCUSSION
This study assessed the knowledge, practices, and attitudes of healthcare providers towards IV fluid administration and stewardship in pediatric intensive care settings in Alexandria. The findings revealed significant knowledge gaps and practice inconsistencies among nurses, physicians, and pharmacists, consistent with regional and international literature.
Regarding nurses' knowledge, results are consistent with Tolera et al. [12], who reported that 42% of nurses in Ethiopian public hospitals had inadequate knowledge of pediatric IV fluid therapy and demonstrated that inadequate knowledge increases the risk of prescribing and administration errors. In the current study, only 35% of nurses correctly answered basic knowledge questions, indicating an even greater knowledge deficit.
Pharmacists in this study demonstrated the lowest confidence in managing IV fluid therapy, with only 7.8% reporting being very confident — despite achieving the highest rate of correct knowledge responses (52%). This discrepancy may reflect a structural barrier: pharmacists in Egyptian public hospitals often have limited involvement in bedside clinical decision-making, reducing opportunities to translate theoretical knowledge into practice. This institutional gap warrants targeted interventions to better integrate clinical pharmacists into PICU stewardship teams.
Similarly, Nasa et al. [11] conducted an international cross-sectional survey and found substantial variability in knowledge and prescribing patterns among healthcare providers, with many lacking awareness of recent guidelines. This aligns with the current study's finding that only 66.1% of nurses and 54.9% of pharmacists were familiar with local or international pediatric IV fluid guidelines, underscoring the urgent need for targeted educational interventions.
Fluid overload was identified as the most common complication by nurses (80.4%) and pharmacists (64.7%). Comparable findings were reported by Teshome et al. [10], where 59.3% of nurses and midwives in Ethiopian hospitals had inadequate IV fluid administration practices, with fluid overload and extravasation being the predominant complications. These findings reinforce the critical need for enhanced stewardship programs with a focus on complication monitoring and prevention.
Training gaps were substantial across all groups. Only 55.4% of nurses and 25.5% of pharmacists had received specific IV fluid stewardship training, compared to 61.9% of physicians. Tolera et al. [12] found a significant association between in-service training and knowledge adequacy, with trained nurses being four times more likely to demonstrate adequate knowledge — strongly supporting the recommendation for structured, regular training programs targeting nurses and pharmacists.
Nasa et al. [11] also highlighted the importance of multidisciplinary stewardship involving all healthcare professional roles in optimizing IV fluid therapy outcomes, consistent with the conclusions of the present study. The identified barriers — lack of time, insufficient guidelines, uncertainty about fluid choice, and difficulty monitoring patients — should be addressed through institutional policy adjustments, dedicated stewardship committees, and resource allocation strategies appropriate to low–middle-income country contexts.
STRENGTHS AND LIMITATIONS
This study provides locally relevant data on a clinically important topic with limited existing literature from the Egyptian pediatric ICU context. The inclusion of three distinct healthcare professional groups enabled meaningful comparative analysis across disciplines. Limitations include the single-region design, reliance on self-reported data which may be subject to social desirability bias, the relatively small physician subgroup (n = 21), and the absence of external questionnaire validation in this specific population. These factors limit generalizability and should be considered when interpreting the findings.
CONCLUSION
Structured fluid stewardship programs integrating physicians, nurses, and pharmacists are essential to improve safety in pediatric IV fluid therapy within Alexandria hospitals. This study identified significant and clinically meaningful knowledge gaps, practice inconsistencies, and training deficits across all healthcare provider groups, with pharmacists and nurses most urgently requiring targeted educational interventions. Barriers to stewardship implementation — including time constraints, insufficient guidelines, and uncertainty in clinical decision-making — must be addressed through institutional policy adjustments, resource allocation, and continuous professional development. Multidisciplinary stewardship committees and regular quality assurance exercises should be established as priority measures to optimize IV fluid therapy outcomes and reduce preventable complications in vulnerable pediatric populations.
ACKNOWLEDGEMENTS
We would like to thank all physicians ,pharmacists and nurses for their participation in our study, Dr Nagwa Mostafa for her effort and continuous support, and Dr Hadeer Hisham for her help. Finally, we would like to thank PharmD board of supervisors at the Faculty of Pharmacy, Alexandria University.
REFERENCES
- Malbrain MLNG, Wong A, Nasa P, Ghosh S. (2021). Introduction to Fluid Stewardship. In: Malbrain MLNG, Wong A, Nasa P, Ghosh S, editors. Rational Use of Intravenous Fluids in Critically Ill Patients. Springer.
- IV Complications. In: Module 1: Advanced Pain Control and Sedation [Internet]. New York: Columbia University Center for Teaching and Learning; [updated 2017 Mar 21].
- Barlow A, Barlow B, Tang N, Shah BM, King AE. (2020). Intravenous Fluid Management in Critically Ill Adults: A Review. Critical Care Nurse.. 40(6):17–27.
- Al-Jawadi HK, Alwiswasi NN. (2021). The role of clinical pharmacists in prescribing IV fluids in Iraqi hospitals. European Journal of Pharmaceutical and Medical Research. 8(9):771-774.
- Ganguly D, Jana S, Sahana M, Jana V, Nandi K, Das H, et al. (2023). Different roles of pharmacists as a healthcare professional: a brief review. International Journal Of Pharmaceutical Sciences and Research. 14(8):3715-3727.
- O'Hare R, Burnett K, Haughey S, Angela C, Edgar L. (2022). The role of the pharmacist in the management of intravenous fluids and electrolytes in adult patients. European Journal of Hospital Pharmacy 29:A30.
- Mishra NT, Prajapati V, Panda S. (2023). The compatibility of intravenous (IV) drugs is a critical aspect of patient care. International Journal of Current Science. 13(1):213–218.
- Abouzeid MI, Elsehrawy MG, Saadoon MM, Nassar HM, Ibrahim AM, Mahmoud AS, et al. (2024). Pediatric nurses' performance enhancement regarding management of quality sensitive nursing indicator: Pediatric IV infiltration in intensive care units. International Journal of Africa Nursing Sciences. 21:100767.
- Mohammed NA, Mohamed MA, Ahmed A. Central venous catheter related complications in Pediatric Intensive Care Unit (PICU). Alex J Pediatr. 2020;33(1):10–6.
- Teshome M, Geda B, Yadeta TA, Mideksa L, Tura MR. (2023). Intravenous fluid administration practice among nurses and midwives working in public hospitals of central Ethiopia: a cross-sectional study. Heliyon. 9(8):e18720.
- Nasa P, Wise R, Elbers PWG, Wong A, Dabrowski W, Regenmortel NV, et al. (2022). Intravenous fluid therapy in perioperative and critical care setting — Knowledge test and practice: An international cross-sectional survey. Journal of Critical Care. 71:154122.
- Tolera GG, Kasaye BM, Abicho TB. (2024). Knowledge and practice towards intravenous fluid therapy in children among nurses in the pediatrics emergency department of selected public hospitals. Scientific Reports.. 14(1):2503.
- Questionnaire about assessment of healthcare staff knowledge about pediatric IV fluids stewardship [Internet]. Google Forms; [cited 2025 Oct 14].